
Most men do not realize there are two types of prostate biopsies. Both procedures share the same goal of sampling prostate tissue precisely enough to confirm or rule out cancer, but they get there through different paths, with different trade-offs.
What Is a Prostate Biopsy?
A prostate biopsy is a way to diagnose prostate cancer. When a PSA test, a digital rectal exam, or a prostate MRI raises enough suspicion, a urologist uses a thin needle to collect small cores of prostate tissue, which a pathologist examines under a microscope to look for cancer cells and assign a Gleason score.
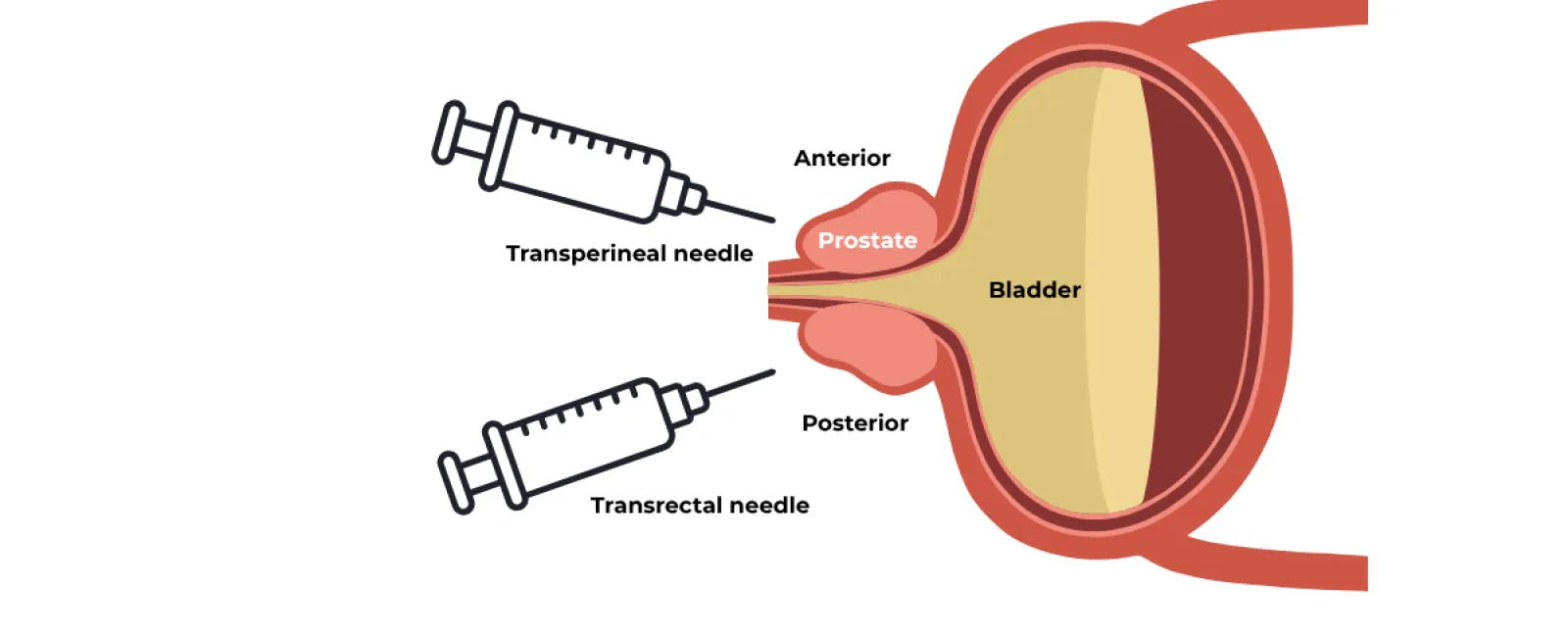
The two main routes into the prostate gland are the transrectal approach, in which the needle passes through the wall of the rectum, and the transperineal approach, in which the needle passes through the perineum, the area of skin between the scrotum and the rectum. Both techniques can be combined with MRI fusion technology to target suspicious lesions identified on imaging, and both are typically performed as outpatient procedures under local anesthesia.
The Two Approaches at a Glance
Before getting into the details, here is how the two prostate biopsy techniques compare side by side:
Transrectal Biopsy (TR) |
Transperineal Biopsy (TP) |
|
Needle entry point |
Through the rectal wall |
Through the perineal skin |
Anesthesia |
Local and/or sedation |
Local and/or sedation |
Procedure time |
10 to 15 minutes |
20 to 30 minutes |
Antibiotic prophylaxis |
Routinely required |
Often optional |
Anterior lesion access |
Limited |
Excellent |
MRI fusion compatible |
Yes |
Yes |
Risk of post-procedure sepsis |
Approximately 3% |
Less than 0.1% |
Transrectal Prostate Biopsy: The Traditional Approach
Transrectal ultrasound-guided biopsy, often called TRUS biopsy, has been the standard prostate biopsy technique for decades. It is short, well-tolerated, and can be performed in an office setting under local anesthesia. However, some patients prefer to get sedation for the procedure.
During the procedure, a small ultrasound probe is inserted into the rectum to visualize the prostate, and a thin biopsy needle is passed through the rectal wall to collect tissue cores from a systematic pattern across the gland. The cores are NOT taken randomly. They are distributed across the sextant peripheral zones where cancer commonly occurs. If MRI imaging has identified suspicious areas in advance, additional targeted cores can be taken from those locations using software-based fusion.
The drawback is anatomical. Every needle pass crosses the rectal wall, and the rectum cannot be sterilized the way skin can. Despite the use of prophylactic antibiotics and antiseptic preparation, gut bacteria, increasingly fluoroquinolone-resistant E. coli, can be carried into the prostate and bloodstream during the procedure. The result is a small but real risk of sepsis that could require hospitalization and IV antibiotics.
Transperineal Prostate Biopsy: The Modern Standard
The transperineal prostate biopsy reaches the prostate by a different route entirely. Instead of crossing the rectal wall, the biopsy needle enters through the perineal skin, which can be sterilized just like any other surgical site. The ultrasound probe still goes in the rectum to provide real-time imaging, but the rectal wall itself is never punctured.
The procedure is performed in roughly twenty to thirty minutes. Due to the setup and positioning required, in addition to the need for the patient to remain still, the procedure is usually performed under sedation.
When combined with MRI fusion guidance, the transperineal approach gives the urologist a precise three-dimensional map of the prostate and allows targeted sampling of any suspicious lesion identified on pre-procedure imaging. Critically, it provides excellent access to the anterior prostate, the front portion of the gland, which is notoriously difficult to reach reliably from the transrectal route and where a meaningful percentage of clinically significant cancers are located.
Head-to-Head: How the Two Compare
Infection Risk and Sepsis
This is where the two prostate biopsy techniques diverge most dramatically. Recent systematic reviews report dramatically lower sepsis rates with transperineal biopsy compared with the historical sepsis rates seen in transrectal biopsy. Several large transperineal series have reported zero cases of sepsis even when antibiotic prophylaxis was omitted entirely.
The implication is meaningful. With rising rates of fluoroquinolone-resistant bacteria across the population, the infection profile of transrectal biopsy has worsened over the last decade, while the transperineal approach has effectively removed the dominant route of bacterial transmission.
Cancer Detection Accuracy
Both approaches detect prostate cancer at broadly similar rates when used for systematic biopsy of the whole gland. The picture changes when targeting matters.
For anterior tumors, those located at the front of the prostate, farthest from the rectum, the transperineal approach has consistently demonstrated better detection. Large comparative studies have reported higher clinically significant cancer detection rates with transperineal compared with transrectal biopsy, with notably stronger anterior tumor detection by the transperineal route.
When MRI fusion is added, several recent studies have shown a meaningful advantage for transperineal fusion biopsy in detecting clinically significant cancer at apical and anterior locations, where higher-grade tumors can otherwise be missed entirely on a standard biopsy.
Patient Experience and Recovery
Both procedures are outpatient. Most men go home the same day and return to normal activity within one to two days. Some mild discomfort, blood in the urine, and blood in the semen are normal after either prostate biopsy and resolve within a few weeks.
The transrectal procedure is shorter and may be slightly more comfortable for patients during the recovery period, as there are less sensory nerve endings in the proximal portion of the rectum. The trade-off is the higher infection risk discussed above. The transperineal procedure takes a bit longer due to equipment and positioning and involves a bit more soreness in the perineal area, but it substantially lowers the risk of post-biopsy infection.
Which Prostate Biopsy Is Right for You?
For most men today, transperineal biopsy with MRI fusion guidance is the more accurate and safer choice. There are situations where the conversation is more individual, however, and the right answer depends on the full clinical picture, your urologist's experience and equipment, and your own priorities.
A transperineal prostate biopsy is especially worth asking about if you have a higher risk of infection or are colonized with fluoroquinolone-resistant bacteria, have had a previous negative transrectal biopsy but a persistently elevated PSA, have suspicious MRI findings in the anterior prostate, are on active surveillance and need ongoing monitoring biopsies, have inflammatory bowel disease or another condition that complicates rectal access, or want to avoid antibiotic prophylaxis where possible.
What matters most is that the conversation about biopsy approach happens before the procedure is scheduled, not after the fact. A biopsy is a one-shot opportunity to get an accurate read on what is happening inside the prostate, and the route used has a direct effect on how confident you can be in the result.
Taking the Next Step With Confidence
If you have been told you need a prostate biopsy, you have more options than you may realize, and the right approach can meaningfully reduce your risk of infection while improving the accuracy of your diagnosis. The urologists at Atlanta Prostate Center specialize in MRI/ultrasound-guided transperineal prostate biopsy, and our team is here to walk you through what to expect and answer any questions you have before you make a decision about your care.
